N8 Casino: Play Online Casino and Sports Betting in India
N8 is an Indian Online Casino with Sports Betting options and a tiered bonus system. The site offers players slots, a live casino with real dealers, as well as sports betting and cyber sports. The site combines a simple interface that is easy to learn and a bright, stylish design that is a pleasure to use.
For those who like to play on mobile devices, there is a handy app available to download directly from the site. Start playing with N8 Casino India today and get a welcome bonus: 100% up to ₹10,000!

About N8 Casino Online Site
N 8 Casino officially opened in 2020. It is now a popular site among Indian players due to its traditional design: bright colors, patterns, symbols, and elements reflecting Indian culture and aesthetics. The site also offers players traditional online card games such as Teenpatti, Andar Bahar, and AK47. In the N8 betting section, players will find betting on Kabbadi and Cricket. The casino section includes over 3,000 games: slots, live online casino, roulette, and blackjack. The site is licensed in India and has a CIN number: U72900DL2016PTC300060.

| Name | N8 Casino |
| Year Founded | 2020 |
| Website Address | n-8.com.in |
| Corporate Identification Number | U72900DL2016PTC300060 |
| Welcome Bonus | 100% up to ₹10,000 |
| Mobile App | Android, iOS |
| Category | Casino, Sports Betting, E-Sports |
| Sports Betting | Cricket, Kabaddi, Football, Basketball, Tennis |
| Deposit Methods | PayTM, PHONEPE, Google Pay, UPI-BONUS2, VIP EXC, USDT |
| Min Deposit | ₹100 |
| Max Deposit | ₹49,999 |
| Support Type | Live Chat, Email |
Step-by-Step Guide to Registering at N8Casino
-
STEP 1

Visit the N8Casino website by entering the official URL in browser;
-
STEP 2

Click on the “Sign Up” button located at the top right corner of the homepage;
-
STEP 3
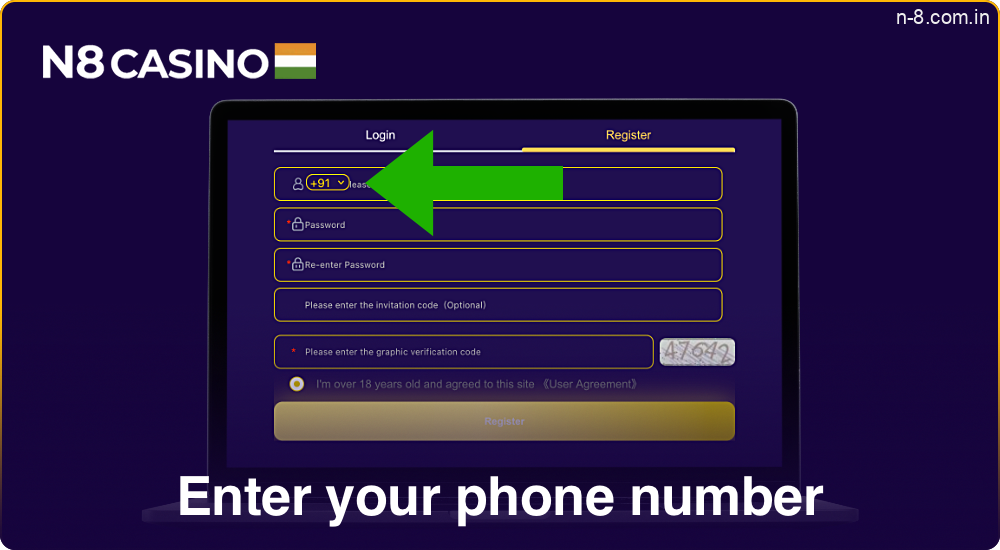
Enter your phone number in the registration form;
-
STEP 4

Create a secure password and agree to the terms and conditions;
-
STEP 5
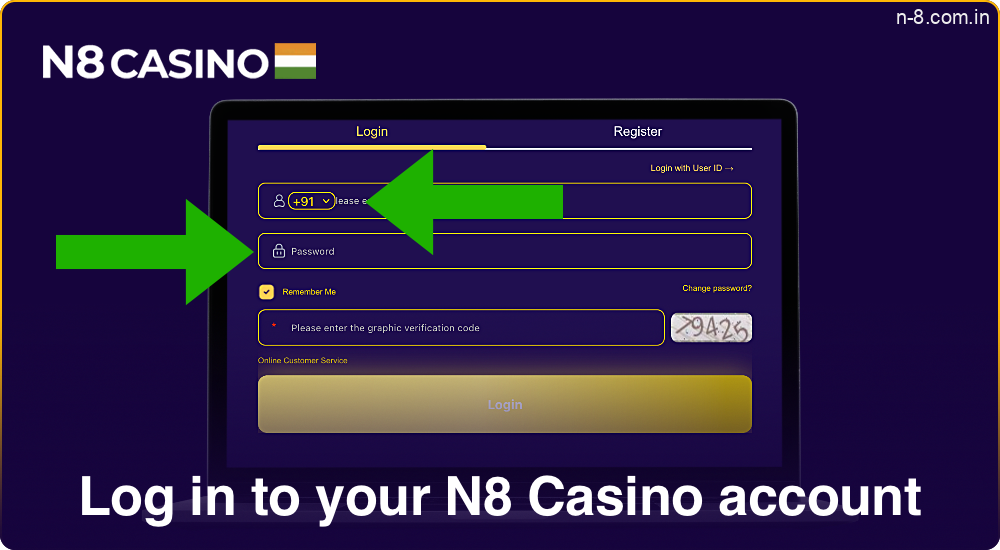
Log in to your N8 account using newly created credentials;
-
STEP 6
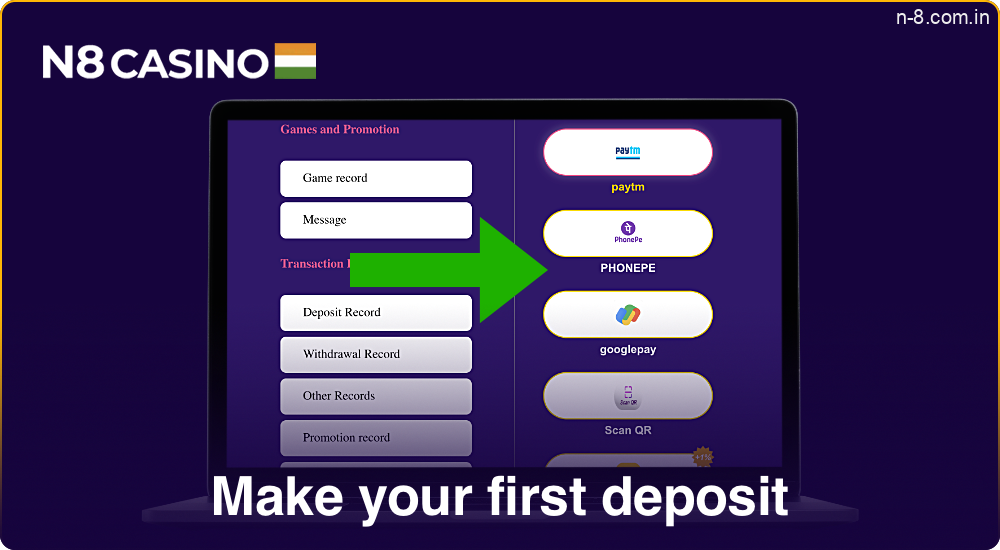
Make first deposit using payment methods like PayTM, PHONEPE or Google Pay;
-
STEP 7
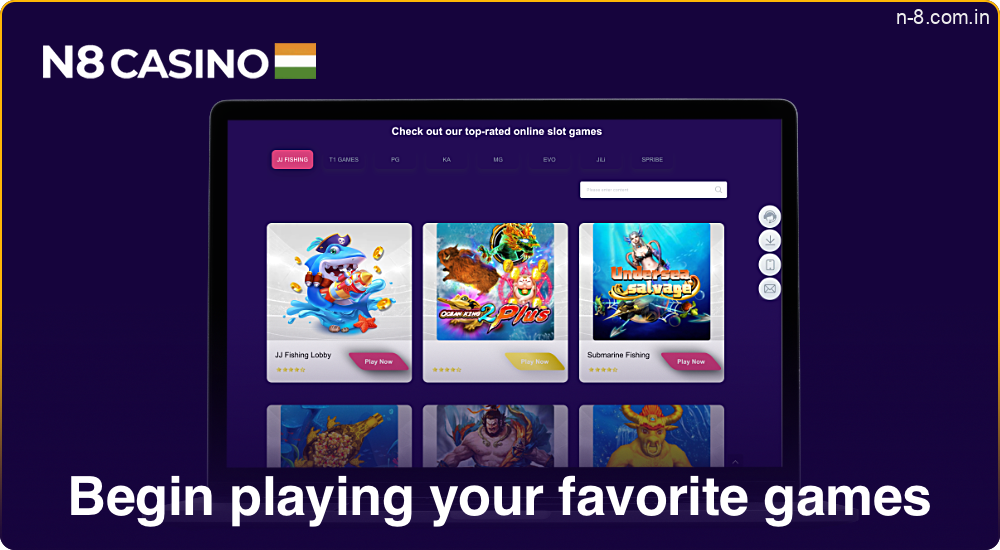
Begin playing your favorite games.
Registering on N8 Casino from a mobile phone is just as straightforward, if not easier. The mobile registration process follows the same steps, optimized for your device’s interface. But keep in mind that registration is not available for users who are below the 18-year old threshold.
How to Log in N8Casino?
Performing an N8 Casino login is very simple and convenient. Just follow the steps below to quickly gain access to your account.
- Open web browser and navigate to the N8 official website;
- Click on the “Login” button located at the top-right corner of the homepage;
- Enter your registered phone number and your password in the respective fields;
- If you have enabled two-factor authentication, enter the code sent to your mobile device;
- Click the “Sign In” button to access your account;
- If you encounter any issues, click on “Forgot Password” to reset your password or contact support for assistance.

Verification
On the N8 Casino games website, verifying your identity is essential to ensure the security of your account and is necessary for making withdrawals. An employee of the site may request a scan of documents to confirm identity. This verification process typically involves:
- Submitting a government-issued ID such as a passport or driver’s license;
- Provide a recent utility bill as proof of address;
- Uploading a clear, color scan of your documents;
- Waiting for the verification team to review your submission;
- Receiving confirmation once your identity has been successfully verified.

Bonuses and Promotions in N8 Casino
N8 offers a variety of bonuses and promotions to enhance the gaming experience for its players. From welcome offers to daily rewards, these bonuses provide extra value and exciting opportunities to maximize winnings. Below are some of the key promotions available to N8 Casino users:
- First Deposit Bonus: Get extra free bonus money equal to 30-100% of first deposit. New customers only;
- Daily Deposit Bonus: Receive a bonus between 5-30% on deposits made each day. Percentage varies by weekday. Must wager deposit + bonus amount before withdrawing;
- Referral Bonus: Invite friends and receive up to 500 per valid referral, plus potential extra bonuses based on referral volume tiers. Friends must sign up and deposit to be valid.

Promo Codes N 8 Casino in 2025
Promo codes at N8 Casino are special codes that provide players with bonuses, such as extra funds for gaming or free spins. These codes can be found on the casino’s website or in newsletters sent to registered users. To activate a promo code, players need to enter it during deposit or in the designated section on the website. Promo codes allow players to boost their balance and increase their chances of winning.

N8: Mobile App in India
The N8 Casino mobile app, available for Android and iOS, offers smooth gameplay, exclusive features like push notifications for promotions, and enhanced performance compared to the mobile site. It supports secure payments, full game access, and regular updates for optimal functionality.
Android App
Here are step-by-step instructions for installing the app on an Android device:
- Open browser and go to the official N8 Casino website;
- Find the “Get Android App” button on the homepage and tap it to download the APK file;
- Go to device settings, and enable “Install from Unknown Sources” to allow the APK to be installed;
- Once the APK is downloaded, open the file and follow the instructions to install the app;
- After installation, open the app, sign in, and start playing your favorite casino games or place bets on sports.

And that’s it! The N8 mobile app should now be successfully installed and ready to use on your Android device.
iOS App
For iOS users, downloading the N8Casino app is quick and easy. Follow these steps:
- Open Safari or any browser on your iPhone or iPad and go to the official N8 Casino website;
- Look for the iOS download option, typically labeled “Get iOS App” on the homepage, and tap it;
- You will be redirected to the App Store. Tap the “Download” button to install the app;
- The app will automatically install on your device. Once it’s done, open the app;
- Sign in with your account or register a new one and enjoy N8 Casino’s games and betting features.

Payment Methods on N8 Casino
N8 Casino offers a wide variety of convenient and secure payment methods for depositing and withdrawing funds. Players can easily manage their accounts using familiar and trusted options, ensuring fast and hassle-free transactions. The following payment methods are available at N8:
- Bank Cards (Visa, Mastercard);
- Electronic Wallets (PayTM, PhonePe, Google Pay);
- UPI Payments (UPI-Bonus2);
- Cryptocurrency (USDT);
- VIP Digital Currency Exchange (VIP EXC).
These options provide flexibility for players to choose the method that suits their preferences and needs, ensuring smooth transactions.

Deposit and Withdrawal Limits
Handling transactions with N8 is easy, thanks to a wide range of payment options. The table below provides a detailed breakdown of each method’s minimum and maximum deposit limits, offering flexibility and convenience for players in India.
| Payment Method | Min Deposit (INR) | Max Deposit (INR) |
|---|---|---|
| PayTM | 500 | 50,000 |
| PhonePe | 1,000 | 100,000 |
| Google Pay | 500 | 100,000 |
| UPI-Bonus2 | 500 | 100,000 |
| VIP EXC | 200 | 50,000 |
| USDT | -* | 100,000 |
- * – USDT (Tether) is a cryptocurrency, and its decentralized nature allows for greater flexibility when it comes to deposits. Since the value of USDT fluctuates with the market, players have the freedom to deposit any amount that suits them. This is why there is no fixed minimum deposit for USDT, making it a versatile option for players looking to use digital currencies.
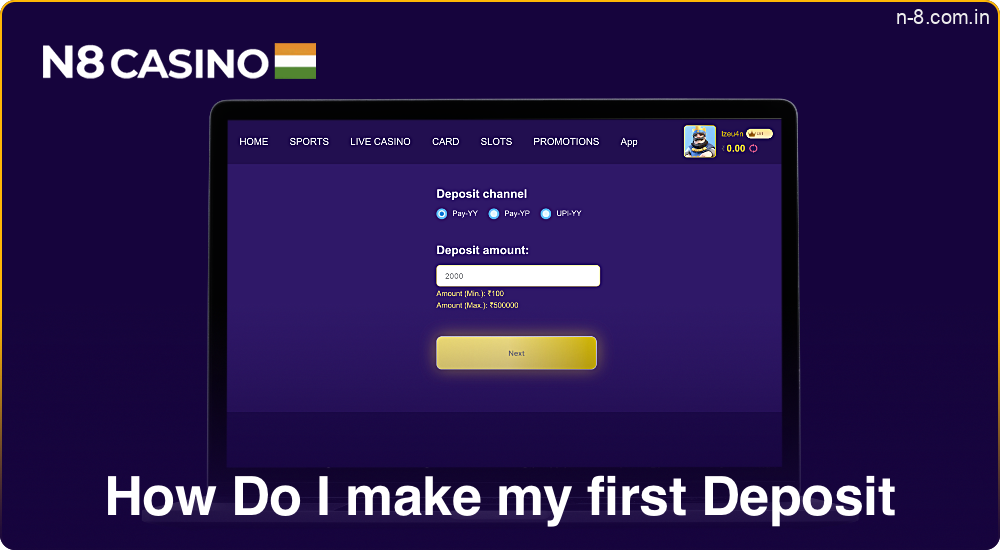
How Do I make my first Deposit?
- Log into your N8 account;
- Navigate to the deposit section;
- Select a payment method such as PayTM, PHONEPE or Google Pay;
- Enter the deposit amount in INR;
- Follow the on-screen instructions to complete the transaction;
- Confirm the deposit in account dashboard.
How to Withdraw Money?
Withdrawing money is simple and secure. Follow these steps to complete your withdrawal:
- Use username and password to access your account dashboard;
- Click on the “Withdraw Funds” option in the main menu;
- Select from options like PayTM, PHONEPE or Google Pay;
- Specify the amount you wish to withdraw in Indian Rupees (INR);
- Input any required information related to your chosen payment method;
- Review details and confirm the withdrawal request;
- Withdrawal will be processed within 3-6 business days, and the funds will be transferred to your selected payment method.

N8 Betting
N8 Sports Betting provides a diverse range of options for sports enthusiasts, offering exciting opportunities to wager on both local and international events. Players can place bets on popular sports, including:
- Cricket;
- Kabaddi;
- Football;
- Tennis.

Cricket
N8 offers a wide range of cricket betting markets to cater to every fan’s preferences, including Main, Match, Session, and Player bets. You can place wagers on the overall match results, specific sessions, or individual player performances. In addition to regular matches, N8 covers major tournaments in India such as:
- Indian Premier League (IPL) – Over 60 matches;
- Ranji Trophy – More than 100 matches;
- Syed Mushtaq Ali Trophy – 150+ matches.
With competitive odds and a user-friendly interface, N8 ensures a top-notch cricket betting experience for every enthusiast.

Kabaddi
Kabaddi enthusiasts can explore a variety of betting markets tailored to enhance their gaming experience. The main kabaddi betting markets include match winners, series winners, and individual player performance. Additionally, bettors can engage in live betting options, allowing wagers during ongoing matches for real-time excitement. N8 offers various betting options, such as head-to-head predictions, total points scored, and specific event occurrences within a match.
N8 covers major kabaddi tournaments in India, including:
- Pro Kabaddi League (PKL) – Over 130 matches;
- National Kabaddi Championship – 50+ matches;
- Federation Cup – 40+ matches.

Football
Football is one of the most popular sports in the world, attracting millions of spectators and fans. Choose from combo mix parlay, live betting, today’s matches, early market opportunities, and more. Supports a range of betting types, including OE & TG, 1×2 & DC, FT & FH CS, HT/FT, FG/LG, mix parlay, and outright bets. Additionally, take advantage of N8 live betting to engage with games in real time. N8 covers popular tournaments in India, including:
- Indian Premier League (IPL) – Over 60 cricket matches;
- Pro Kabaddi League (PKL) – More than 130 kabaddi matches;
- Ranji Trophy – Over 100 cricket matches;
- Syed Mushtaq Ali Trophy – 150+ cricket matches.

Tennis
The main tennis betting markets include match winner, set betting, and total games. Additionally, N8 provides features like live betting and cash-out, allowing you to place bets in real time and secure winnings before the match concludes. N8 covers key tennis tournaments in India, including:
- Chennai Open – Over 40 matches;
- Bengaluru Open – More than 50 matches;
- Tata Open Maharashtra – 60+ matches.

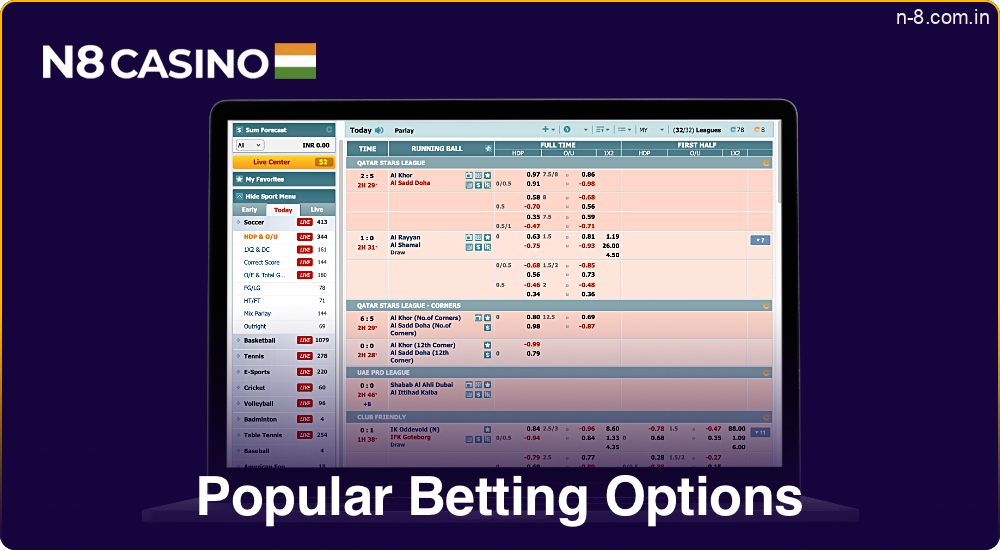
Popular Betting Options
This brand offers a wide range of popular betting options to cater to every player’s preferences. From pre-match betting to live betting, these options offer flexibility and excitement. Below are some of the most commonly used betting features available on the platform:
- Live Betting: Engage in real-time wagers on ongoing matches and events;
- Line (Prematch): Place bets on events before they start with diverse lines;
- Outright Betting: Bet on the overall outcome of leagues or tournaments through N8’s outright options.
Types Of Bets
At N8 bet, bettors have access to a diverse range of bet types designed to enhance their wagering experience. Understanding these different types can significantly improve chances of success and make betting more enjoyable.
- Single – A bet on one selection to win independently, offering straightforward wagering;
- Combo – Combines multiple selections where all must win for a payout, increasing potential returns;
- System (Express) – Provides multiple combinations of selections, allowing flexibility and broader betting opportunities.

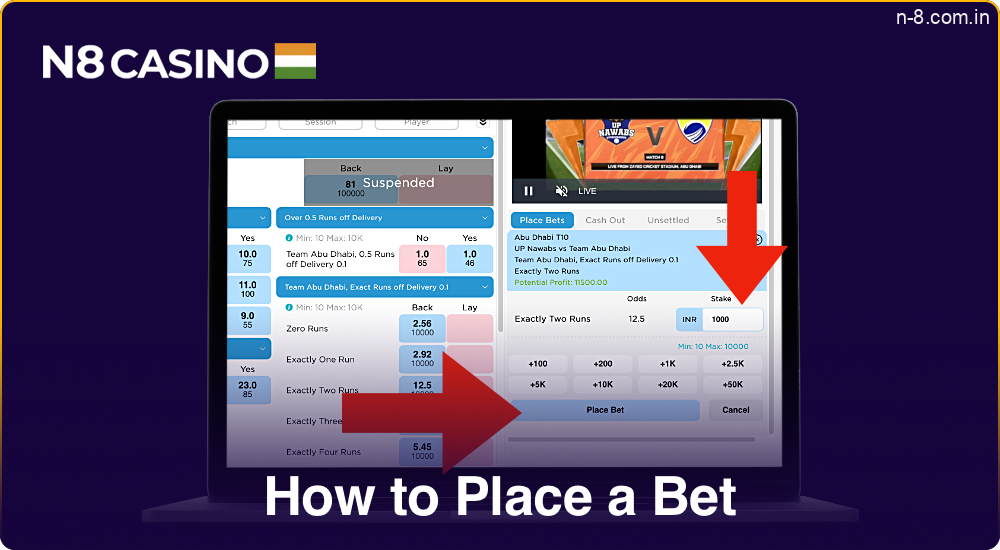
How to Place a Bet?
Placing a bet is simple with betting N8. Follow these steps:
- Visit the N8 website;
- Sign up by providing necessary personal details;
- Add money to your account using payment methods such as PayTM, PHONEPE or Google Pay;
- Browse through the available sports or events and choose one you want to bet on;
- Decide stake, choose bet type, and confirm the bet through.
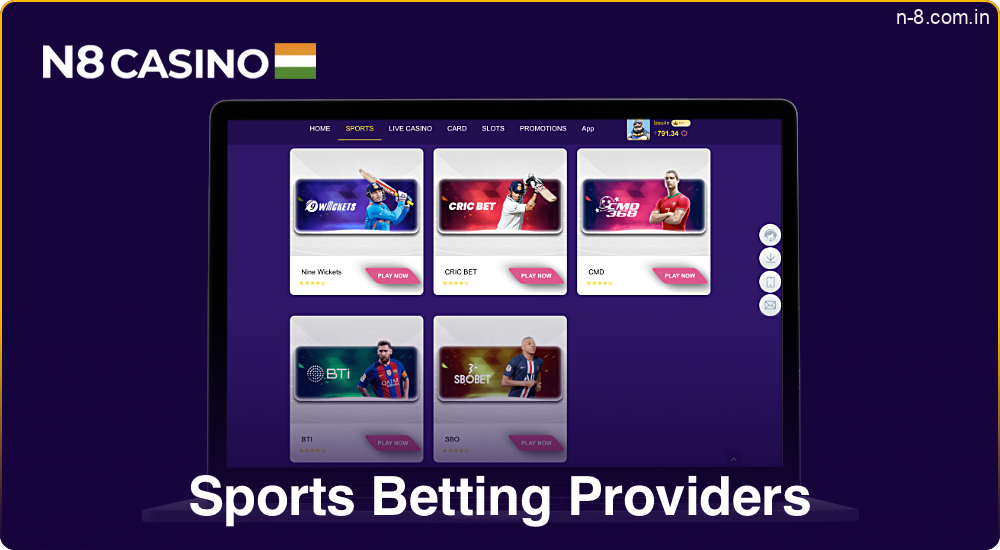
Sports Betting Providers
Here are some of the leading sports betting providers featured on N8:
- Nine Wickets is renowned for competitive cricket odds and prop bets, making it a favorite among bettors;
- Cric Bet offers a wide selection of cricket-related betting options, ensuring diverse wagering opportunities;
- CMD provides detailed cricket analysis and accurate predictions to inform betting decisions;
- BTI focuses on delivering the best betting tips across major sports in India, including cricket, football, and kabaddi;
- SBO boasts a user-friendly platform and competitive odds, enhancing the overall betting experience.
Virtual Sports
On the N8 website, virtual sports are a simulation of real sporting events using computer algorithms and graphics. Players can place bets on popular virtual disciplines such as:
- Football;
- Horse racing;
- Tennis.
Match takes place every few minutes, providing quick results and continuous action. Unlike real matches, outcomes in virtual sports are determined by a random number generator, making them unpredictable and fair. With realistic graphics, dynamic gameplay, and competitive odds, virtual sports on N8 offer an excellent alternative for those who prefer fast and frequent betting, available at any time.

N8 Online Casino Portfolio
Casino N8 offers an exciting and varied selection of games for every type of player. Whether you love classic table games or modern slots, this site has something for everyone. Below is an overview of the different categories of games available, choose what you like best and start having fun:
- Slots: Choose from 500+ a wide variety of online slots with engaging themes;
- Blackjack: Enjoy classic and modern blackjack variants;
- Roulette: Spin the wheel in multiple roulette options;
- Poker: Test your skills with various poker games;
- Baccarat: Experience the elegance of baccarat;
- Video Poker: Combine strategy and luck in video poker;
- Live Dealer Games: Interact with live dealers for an immersive experience;
- Jackpot Games: Play for the chance to win big jackpots.

Slots
N8 Casino offers a variety of slots from leading developers such as PG, KA, MG, EVO, and JiLi, giving players a wide selection of engaging games with high-quality graphics and unique features. The slot collection includes popular games with high RTPs and exciting bonuses, as shown in the table:
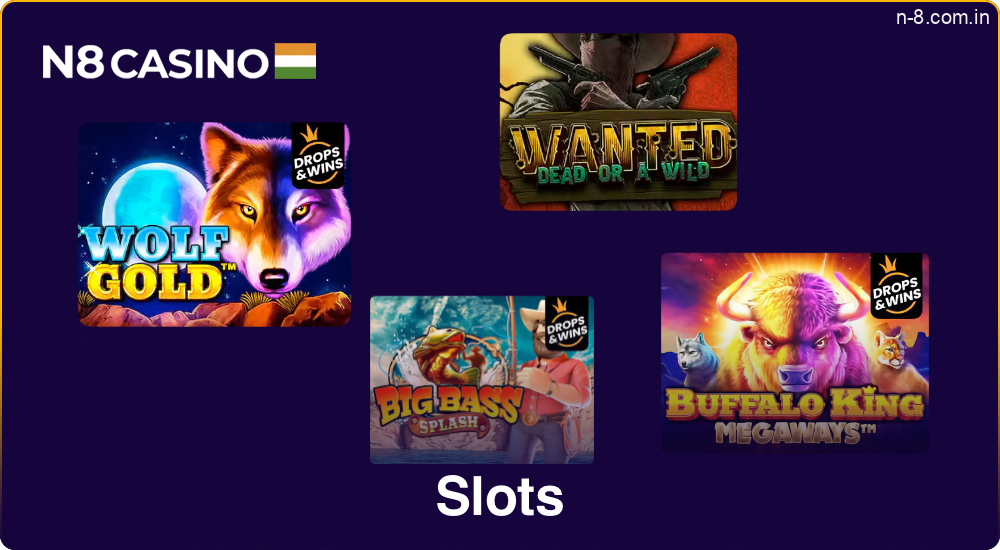
| Title Slot | RTP | Main Advantage |
|---|---|---|
| Wolf Gold | 96.01% | High volatility, big wins |
| Wanted Dead or a Wild | 96.38% | Immersive Western theme |
| Buffalo King Untamed Megaways | 96.50% | Megaways, many pay lines |
| Big Bass Splash | 96.71% | Fishing theme, bonus rounds |
These games offer not only a variety of themes but also high winning chances thanks to well-designed mechanics and appealing bonus features.
Card Game
Online card games are hugely popular in India, offering exciting and immersive experiences for players. RTP for these card games is usually higher than in slots, with many offering over 97%. This is because games like Rummy and Teenpatti involve some level of skill, allowing players to make decisions that can affect the outcome. In slots, everything is based on luck, but in card games, players have more control, which leads to better chances of winning. Popular card games include:

| Title game | RTP | Main Advantage |
|---|---|---|
| Teenpatti | 97.00% | Popular card game |
| AK47 | 96.20% | Unique AK47 twist |
| Andar Bahar | 97.85% | Simple, exciting bets |
| Rummy | 97.50% | Classic strategy game |
| Teenpatti 20-20 | 96.80% | Fast-paced Teenpatti |
Live Casino in N8
N8 Live Casino delivers a top-tier online gambling experience with a diverse selection of live games hosted by professional dealers, offering players a fully immersive and authentic casino atmosphere. Here’s a closer look at each game available:
- Live Blackjack;
- Live Roulette;
- Live Andar Bahar;
- Live Baccarat;
- Live Game Shows;
- Live Sic Bo;
- Live Dragon Tiger;
- Live Teen Patti.
Each game at N8 Live Casino combines realistic gameplay with smooth streaming, letting players enjoy the excitement of live action from the comfort of home.

Legitimacy and Trustworthiness
N8 Casino operates under a licensed and regulated framework, holding a valid license number CIN: U72900DL2016PTC300060, ensuring a secure environment for all users in India. The platform adheres to stringent standards set by independent authorities, which guarantees fair play in all games. Players’ personal information and financial details are safeguarded, ensuring the safety of players’ funds at all times. Regular audits are conducted to maintain transparent operations, further enhancing trust.
Additionally, N8 is known for prompt payouts and a user-friendly interface, making the experience smooth and reliable. With responsive customer support available for any inquiries, players can feel confident in the casino’s commitment to maintaining high standards of trust and security.

Why is a CIN License Important for Players?
N8 operates under a valid CIN license number: U72900DL2016PTC300060. But what exactly is a CIN number, and why is it important for players? A Corporate Identification Number (CIN) is a unique number assigned to companies registered in India. It serves as proof that a company is legally registered and operating under Indian laws. The CIN number for N8 Casino is a key identifier that ensures the platform operates transparently and adheres to all legal requirements.
- Trust & Security: The CIN license confirms that N8 is a legitimate business, providing players with a safe and regulated environment for online gaming and betting;
- Legal Compliance: Having a CIN ensures that N8 adheres to all local and national laws in India, protecting players from fraudulent activities;
- Transparency: With a CIN number, players can easily verify the legitimacy of N8, ensuring the platform’s operations are open and trustworthy.

Responsible Gaming
The N8 gambling site places a strong emphasis on responsible gaming, ensuring that players can enjoy their experience in a safe and controlled environment. The platform provides several tools to help users manage their gambling habits effectively. Features such as deposit limits, session time reminders, and self-exclusion options allow players to set boundaries and maintain control over their gaming activity.
To further support player well-being, the site offers access to educational resources and professional organizations that assist in preventing and addressing gambling-related issues. The platform is committed to fairness and transparency, consistently promoting a balanced approach to gaming. By adopting industry best practices, the site ensures that players can enjoy entertainment without compromising their safety or well-being.

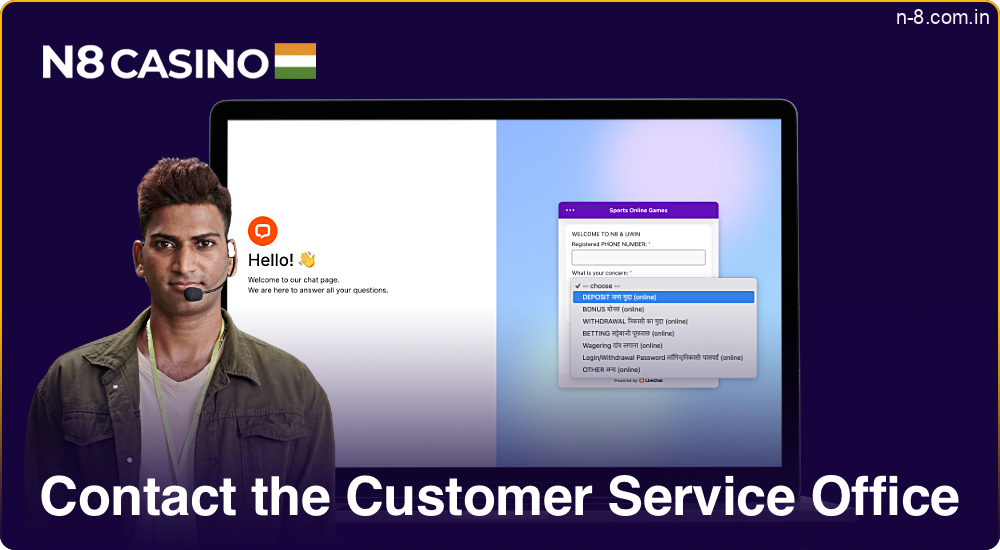
Contact the Customer Service Office
You can contact the customer service N8 office through various methods to ensure a seamless experience:
- Live chat on website;
- Email support at [email protected];
- Phone at +91-1234-567890.
FAQ
How to Register on the N8 Casino Website?
To register on the N8 Website, visit their website and click “Sign Up.” Enter your details, phone number, and complete the registration. Once registered on N8, you can access all features and services.
What Bonuses Does N8 Casino Offer for New players?
N8 provides new players with a generous welcome bonus 100% up to ₹10,000 upon registration. Additionally, N8 offers a deposit match bonus to enhance initial investment, ensuring a strong start with the platform.
How Do I Deposit To My N8 Account?
To deposit to N8 account, use payment methods such as PayTM, PHONEPE or Google Pay.l. Log in N8 account, navigate to the deposit section, select your preferred method, enter the amount in INR, and follow the on-screen instructions to complete the transaction.
What Types of Sports Betting Does N8 Offer?
N8 Casino India sports betting provides a variety of sports betting options including cricket, football, basketball, tennis, and more. Players can enjoy live betting, pre-match betting, and special bets tailored to enhance the betting experience.
Does N8 Casino Have a Mobile App and How Do I Download It?
N8 offers a mobile app available for both Android and iOS devices. To download the app, visit the official N8 site and tap the “Get” button. Follow the on-screen instructions to install and start using the app.
Is It Safe to Play and Bet at N8?
Playing and betting at N8 is safe due to its secure platform and reliable N8 betting options. The site uses advanced encryption to protect data, offers various payment methods like PayTM or Google Pay, and is licensed by reputable authorities, ensuring a trustworthy gaming experience: CIN: U72900DL2016PTC300060.